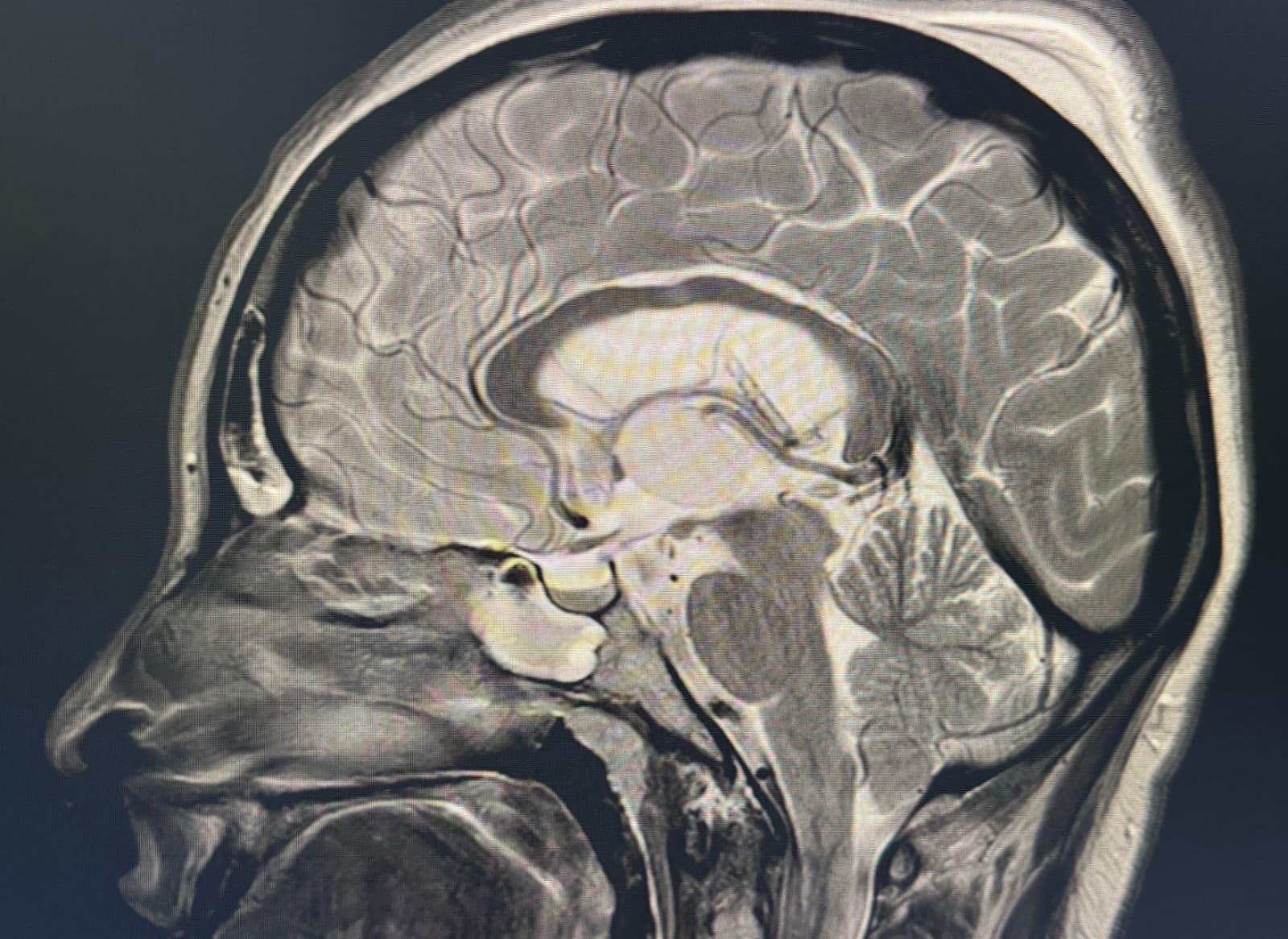
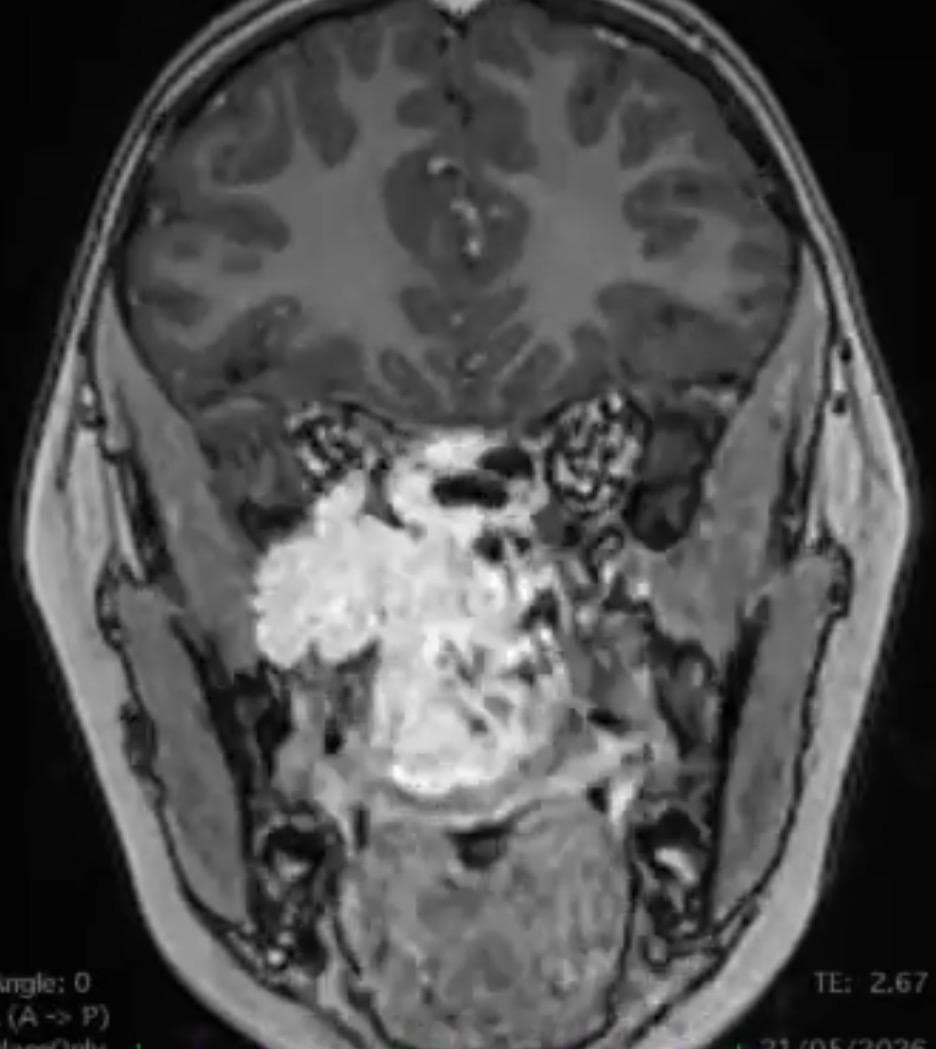
Chordomas are rare tumors arising from embryonic remnants of the notochord. They are locally aggressive, recurrent tumors that invade both bony and soft tissue. The biological nature of chordomas makes them midline central tumors, most commonly located at the skull base and the sacrum. Symptoms depend on location — in this description we will focus on those at the skull base.
They originate in the bony tissue of the clivus, and their growth can extend either outward — toward the paranasal sinuses, pharynx, paravertebral muscles or the first cervical vertebrae — or inward into the cranium, involving cranial nerves or the brainstem. Clinically they present with headache, cervical pain, double vision, tongue mobility disorders, swallowing difficulties, hoarseness, gait instability, etc.